You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Morton's Neuroma?
- Thread starter calnebarefoot
- Start date
I don't have Morton's Neuroma. I did have bunions, but I've managed to straighten them after 3 years of stretching and exercises. In the process, I've restored some of the natural spacing between the toes. (The bunion bumps and bursal sacs remain, but I'm hoping that they might improve after a few more years.)
I'm no foot expert, but I've learned a lot from other people's experiences, so I'm sharing mine. After all, isn't that what forums are for?
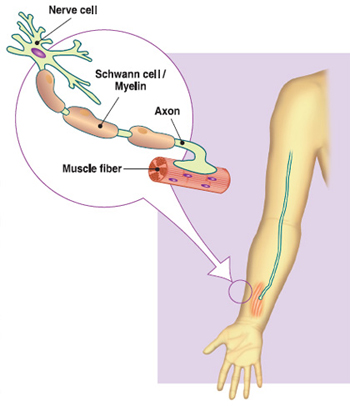
I have tried Yoga Toes. They were pretty tight at first, and offer a light stretch now. I got to the point where I could sleep with them at night, but ended up kicking them off when they became uncomfortable. They also woke me up whenever I moved my feet under the sheets, as the rubber sticks to the sheets. I think that the manufacturer doesn't recommend them overnight, because as far as I can tell from diagrams, the blood vessels and nerves run between the toes. If the circulation is cut off and someone doesn't kick them off, they could wake up with gangrenous toes!
I have not tried Correct Toes, but I have tried similar individually sold spacers. They don't stay in place without socks and shoes. I slowly worked up to the point where I'd have 2-3 between the toes 1-4. I did not intend to increase the spacing between all of my toes, but had to add more spacers to the rest of the toes, while my big toes were straightening out. If I only put spacers between my 1st and 2nd toes, my big toes would have pushed the smaller toes off to the side, making them crooked!
Improving the flexibility using the spacers was only the first step. After that, I worked on further stretching manually and strengthing the muscles. I tried splaying my toes as much as possible. I wasn't able to do much as first, but after many months and more stretching, I was able to strengthen the abductor hallucis, so now I can at least abduct the big toes into a straight position.
I also noticed that my left foot which had the more severe bunion was narrower and had less muscle tone than the right foot. After straightening out the bunion, my left foot is now widening out more and starting to catch up in development.
I also noticed that I was able to put more weight on my right big toe than the left one. I noticed when I tried to do a releve to demi-pointe that the big toe on the left would collapse towards the smaller toes. It seemed that the muscles were still a bit weak, so I still work on this trying to keep the big toe splayed.
I also take calcium supplements, and have done so since a professor suggested it to everyone in class years ago for general health. He taught the medical students, too. So, I took him at his word. I don't know if it reduces the risk of fractures or not.
Lastly, I've been doing some gravel training recently. Probably not good for those with MN, but I feel that it's helped with flexibility. After all, one needs to land softly with flexible feet on gravel. I think that part of why Ken Bob recommends starting with gravel.
This is all still a work in progress, but I no longer need to wear the toe spacers or Yoga Toes. I do wear a bunion splint at night to keep the big toes straight. Incidentally, they are the same bunion splints that I used before I started this process. Only now, I have them set at the fully straight setting, rather than mostly crooked!
I'm no foot expert, but I've learned a lot from other people's experiences, so I'm sharing mine. After all, isn't that what forums are for?
I have tried Yoga Toes. They were pretty tight at first, and offer a light stretch now. I got to the point where I could sleep with them at night, but ended up kicking them off when they became uncomfortable. They also woke me up whenever I moved my feet under the sheets, as the rubber sticks to the sheets. I think that the manufacturer doesn't recommend them overnight, because as far as I can tell from diagrams, the blood vessels and nerves run between the toes. If the circulation is cut off and someone doesn't kick them off, they could wake up with gangrenous toes!
I have not tried Correct Toes, but I have tried similar individually sold spacers. They don't stay in place without socks and shoes. I slowly worked up to the point where I'd have 2-3 between the toes 1-4. I did not intend to increase the spacing between all of my toes, but had to add more spacers to the rest of the toes, while my big toes were straightening out. If I only put spacers between my 1st and 2nd toes, my big toes would have pushed the smaller toes off to the side, making them crooked!
Improving the flexibility using the spacers was only the first step. After that, I worked on further stretching manually and strengthing the muscles. I tried splaying my toes as much as possible. I wasn't able to do much as first, but after many months and more stretching, I was able to strengthen the abductor hallucis, so now I can at least abduct the big toes into a straight position.
I also noticed that my left foot which had the more severe bunion was narrower and had less muscle tone than the right foot. After straightening out the bunion, my left foot is now widening out more and starting to catch up in development.
I also noticed that I was able to put more weight on my right big toe than the left one. I noticed when I tried to do a releve to demi-pointe that the big toe on the left would collapse towards the smaller toes. It seemed that the muscles were still a bit weak, so I still work on this trying to keep the big toe splayed.
I also take calcium supplements, and have done so since a professor suggested it to everyone in class years ago for general health. He taught the medical students, too. So, I took him at his word. I don't know if it reduces the risk of fractures or not.
Lastly, I've been doing some gravel training recently. Probably not good for those with MN, but I feel that it's helped with flexibility. After all, one needs to land softly with flexible feet on gravel. I think that part of why Ken Bob recommends starting with gravel.
This is all still a work in progress, but I no longer need to wear the toe spacers or Yoga Toes. I do wear a bunion splint at night to keep the big toes straight. Incidentally, they are the same bunion splints that I used before I started this process. Only now, I have them set at the fully straight setting, rather than mostly crooked!









As part of my shoemaking adventure, I've measured my feet. They are both 10.25 inches long. My right foot has a max toe splay of 5.5 in. The left (which has the worse bunion) is 5 in. I never took pre measurements, but I'm fairly confident that I've increase not only the toesplay, but also the spacing between my metatarsals.
Despite logging 800 barefoot and 200 minimalist miles, most of this improvement occured after that, over the past year when I made the effort to try to splay my toes all the time to try to improve my bunions.
I think that it's also possible that the gravel training has helped in terms of doing some myofascial release, as the splay on my left foot has improved by 0.5 in over the past few weeks.
Despite logging 800 barefoot and 200 minimalist miles, most of this improvement occured after that, over the past year when I made the effort to try to splay my toes all the time to try to improve my bunions.
I think that it's also possible that the gravel training has helped in terms of doing some myofascial release, as the splay on my left foot has improved by 0.5 in over the past few weeks.
good news!!!COrrect toes have sorted it out.
Will start barefoot running again soon (lots of rain in UK at the minute....)
Will start barefoot running again soon (lots of rain in UK at the minute....)
Maybe you caught it early, while it was reversible?
Isn't restoring function through proper alignment, strengthening, balance of opposing muscles, and promoting flexibility to allow the body to heal itself some of the underlying principles of osteopathy, chiropractic, body work, and physiotherapy?
Hey, if my bone spur is being resorbed, why can't Morton's Neuroma be reversible in the early stages?
http://www.thebarefootrunners.org/index.php?posts/149430
Remove the offending agents and perhaps the body can heal itself!
Isn't restoring function through proper alignment, strengthening, balance of opposing muscles, and promoting flexibility to allow the body to heal itself some of the underlying principles of osteopathy, chiropractic, body work, and physiotherapy?
Hey, if my bone spur is being resorbed, why can't Morton's Neuroma be reversible in the early stages?
http://www.thebarefootrunners.org/index.php?posts/149430
Remove the offending agents and perhaps the body can heal itself!
As you know, MN is basically scar tissue that's built up around the nerve sheath over time from the nerve being compressed between the metatarsals.
I have some members at MN Talk who have taken remedies to help their bodies to reabsorb the scar tissue, and I can give you the recipe if you wish, who swear that these products worked and that they are neuroma-free now because of it.
I have other members who claim that wearing toe spacers or some certain footwear did the trick.
But what I have learned is that many, many of the cases that are diagnosed as MN are actually just enlarged, inflamed nerves. It's quite sad really. These people go through all the motions of having and treating MN, sometimes up to surgery, only to find out that they didn't have MN after all.
Dr. Dellon developed a procedure where he scraps the scar from the nerve leaving the nerve in tact, which is most important. He will either do this procedure first or a nerve decompression where he cuts the tendon freeing the nerve from being entrapped between the mets. When he gets a patient like me though, where the neuromas grew back into stumps after having the traditional neurectomy surgeries, he has to correct that by cutting into the arch(es), resectioning the stump(s) from the nerve, dividing the nerve branches, then reimplanting them into arch muscle.
Does the body then reabsorb the stump neuroma? I have been told yes and no by different doctors. I just asked the PA, PC at my bone and joint doctor's office, and he said no. What can you find in studies that state otherwise, if you will please?
I have some members at MN Talk who have taken remedies to help their bodies to reabsorb the scar tissue, and I can give you the recipe if you wish, who swear that these products worked and that they are neuroma-free now because of it.
I have other members who claim that wearing toe spacers or some certain footwear did the trick.
But what I have learned is that many, many of the cases that are diagnosed as MN are actually just enlarged, inflamed nerves. It's quite sad really. These people go through all the motions of having and treating MN, sometimes up to surgery, only to find out that they didn't have MN after all.
Dr. Dellon developed a procedure where he scraps the scar from the nerve leaving the nerve in tact, which is most important. He will either do this procedure first or a nerve decompression where he cuts the tendon freeing the nerve from being entrapped between the mets. When he gets a patient like me though, where the neuromas grew back into stumps after having the traditional neurectomy surgeries, he has to correct that by cutting into the arch(es), resectioning the stump(s) from the nerve, dividing the nerve branches, then reimplanting them into arch muscle.
Does the body then reabsorb the stump neuroma? I have been told yes and no by different doctors. I just asked the PA, PC at my bone and joint doctor's office, and he said no. What can you find in studies that state otherwise, if you will please?
This is all that I could find.
http://www.ncbi.nlm.nih.gov/m/pubmed/11777237/
For this first link, I find it interesting that this wasn't Dellon's study, or he wasn't a part of it. He developed the procedure. He did tell me that he and others did a study on the link to tarsal tunnel syndrome and found that 50% of the patients who suffer with MN also suffer with TTS, so basically the same thing this study has found...which is nice when they all line up the same.
I have yet to learn what the exact link between the two is though. Why does this happen?
Maybe this?
http://emedicine.medscape.com/article/1236852-overview#6
http://emedicine.medscape.com/article/1236852-overview#6
The double-crush phenomenon originates from work published by Upton and McComas in 1973. The hypothesis behind this phenomenon may be stated as follows: Local damage to a nerve at one site along its course may sufficiently impair the overall functioning of the nerve cells (axonal flow), such that the nerve cells become more susceptible to compression trauma at distal sites than would normally be the case.
The nerves are responsible for transmitting afferent and efferent signals along their length, and they are also responsible for moving their own nutrients, which are essential for optimal functioning. The movement of these intracellular nutrients is accomplished through a type of cytoplasm within the nerve cell called axoplasm (referring to cytoplasm of the axon). The axoplasm moves freely along the entire length of the nerve. If the flow of the axoplasm (ie, axoplasmic flow) is blocked, the nerve tissue that is distal to that site of compression is nutritionally deprived and more susceptible to injury.
Maybe this? http://emedicine.medscape.com/article/1236852-overview#6
The double-crush phenomenon originates from work published by Upton and McComas in 1973. The hypothesis behind this phenomenon may be stated as follows: Local damage to a nerve at one site along its course may sufficiently impair the overall functioning of the nerve cells (axonal flow), such that the nerve cells become more susceptible to compression trauma at distal sites than would normally be the case.
The nerves are responsible for transmitting afferent and efferent signals along their length, and they are also responsible for moving their own nutrients, which are essential for optimal functioning. The movement of these intracellular nutrients is accomplished through a type of cytoplasm within the nerve cell called axoplasm (referring to cytoplasm of the axon). The axoplasm moves freely along the entire length of the nerve. If the flow of the axoplasm (ie, axoplasmic flow) is blocked, the nerve tissue that is distal to that site of compression is nutritionally deprived and more susceptible to injury.
Thanks, Sid. I will read the entire article shortly, and likewise, share it with MN Talk.
I wish they would specifically say that the axo travels in both directions. For example, my feet in the ball of foot region and three center toes are often blue. The nerves are responsible for temperature control. My feet know they are blue and cold, but my brain doesn't. There is a disconnect there, due to the severing, so the signals are not traveling in both directions along that neuro path.
https://www.dartmouth.edu/~humananatomy/part_1/chapter_3.html
Peripheral nervous system
A nerve is a collection of nerve fibers that is visible to the naked eye. The constituent fibers are bound together by connective tissue. Each fiber is microscopic in size and is surrounded by a sheath formed by a neurilemmal cell (comparable to the glial cells of the central nervous system). Hundreds or thousands of fibers are present in each nerve. Thus, according to the number of constituent fibers, a nerve may be barely visible, or it may be quite thick. A nerve as a whole is surrounded by a connective tissue sheath, the epineurium. Connective tissue fibers run inward from the sheath and enclose bundles of nerve fibers. Such bundles are termed fasciculi (funiculi); the connective tissue that encloses them is called perineurium. Very small nerves may consist of only one fasciculus derived from the parent nerve. Finally, each nerve fiber and its neurilemmal sheath are enclosed by a connective tissue sheath termed endoneurium.
Peritoneal nerve fibers may be classified according to the structures they supply, that is, according to function. A fiber that stimulates or activates skeletal muscle is termed a motor (efferent) fiber. A fiber that carries impulses from a sensory ending is termed a sensory (afferent) fiber. Fibers that activate glands and smooth muscle are also motor fibers, and various kinds of sensory fibers arise from endings in viscera. Consequently, a more detailed classification of functional components is sometimes required.
Finally, someone who gets it! I thoroughly enjoyed reading an article from someone who cares about his patients and doesn't just want to cut or freeze the problem away, as he knows that doesn't work. I also notice he referenced Dellon's studies a few times. Great find!



After looking at the before and after photos, I'm going to agree. http://www.thebarefootrunners.org/index.php?posts/150119But what I have learned is that many, many of the cases that are diagnosed as MN are actually just enlarged, inflamed nerves. It's quite sad really. These people go through all the motions of having and treating MN, sometimes up to surgery, only to find out that they didn't have MN after all.
I'm not sure if fibrosis might improve after 2, 5, 10, 20 years, such as scars from childhood injuries. However, it seems unlikely that severe fibrosis would go away any time soon.
My fibrosis, along with the nerves, were cut out. sigh. Too bad I didn't know what I know now, or I would have done differently.
What before and afters are you talking about?
What before and afters are you talking about?
Surgical photos, A & B. That nerve looks completely encased in fibrosis, that's not going to go away by itself anytime soon.
http://radiology.casereports.net/index.php/rcr/article/viewarticle/458/797
http://radiology.casereports.net/index.php/rcr/article/viewarticle/458/797